JAK Inhibitors for Hair Loss: Ultimate Guide
New research from the last few years found that a class of drug called JAK inhibitor has shown potential in addressing alopecia areata.
Given that there are limited treatment options available for this form of hair loss, this may prove to be a game changer.
In addition, there is evidence suggesting that other alopecia — including androgenetic alopecia and telogen effluvium — may also benefit from this class of drug.
This article will briefly explore the mechanism behind JAK inhibitors and review a few studies behind the drug.
What is JAK Inhibitor?
Janus kinase, or JAK for short, is a group of enzymes comprised of JAK1, JAK2, JAK3 and tyrosine kinase 2 (TYK2). They are located within the cell, but on receptors that are present on the cellular surface.
When immune responses need to be coordinated in the body, molecules called cytokines seek and bind to the cell receptor that activates JAK.
With the help of other molecules, JAK transmits the instruction to the cell’s nucleus, where it is processed.
The activation of JAK and its corresponding signaling pathway are necessary for host defenses and immunoregulation, such as the production of white blood cells and obstruction of viral replication, to initiate.
However, it can backfire in cases when it overreacts and causes unnecessary inflammation and immune responses.
Janus kinase inhibitor, also known as JAK inhibitors or jakinibs, is a class of medicine that blocks JAK from activating, thus disrupting the overactivation of immune cells.
Currently, two JAK inhibitor drugs have been approved by the FDA: ruxolitinib and tofacitinib.
Ruxolitinib (Jakafi) was approved in 2011 as an intervention drug for treating myelofibrosis, a rare form of cancer that compromises the bone marrow.
Tofacitinib (Xeljanz) was approved in 2012 to treat patients with moderate — severe rheumatoid arthritis.
Both are being tested in clinical trials for the treatment of plaque psoriasis and — you guessed it — alopecia areata.
A Serendipitous Discovery
JAK inhibitors as a possible drug for treating alopecia areata only started to gain traction in 2014 through a study by Dr. Brett King, a dermatologist and associate professor at Yale University.
Dr. King was evaluating and managing the treatment of a 25-year-old male patient, who had a severe form of plaque psoriasis that had begun 5 years earlier.
In addition to psoriasis, the patient reported a history of alopecia areata, which started at the age of 2 and progressed to alopecia universalis by age 18.
Based on prior research, Dr. King surmised that JAK inhibitors has myriad effects on T-lymphocytes, and can therefore target both the plaque psoriasis and the alopecia universalis.

The first 2 months of tofacitinib at 5 mg twice daily showed some mild improvements in psoriasis, with noticeable signs of partial regrowth on the scalp and face. The dose was then increased to 10 mg in the morning and 5 mg at night, a total of 15 mg daily.
While the tofacitinib provided substantial improvements to the plaque psoriasis, no one anticipated its dramatic response to the patient’s hair.
In only three months after the dose increase, there was complete regrowth of the scalp hair along with regrowth of eyebrows, eyelashes, facial hair, and axillary hair.
A few months later, Christiano and her team of researchers from Columbia University Medical Center also produced similar results in three male patients with alopecia areata.
Like Dr. King’s patient, each subject recovered a full bed of scalp hair within five months of the start of treatment.
The phenomenal response from these two studies spurred headlines and piqued the interest of both the hair loss and biomedical community.
More research has since been conducted, offering possible hypothesis on JAK inhibitors’ ability to effectively target areata alopecia.
JAK Inhibitors can Prevent and Reverse Alopecia Areata
Alopecia areata (AA) is an autoimmune disease resulting from damage to the hair follicle by T cells.
Of that group, approximately 20 percent have alopecia totalis or alopecia universalis.
Normally, the immune system protects you from infection and illnesses by eliminating any foreign bodies that are not your own. This can include harmful bacteria, viruses, and parasites.
In alopecia areata, hair follicles from the scalp and other areas of the body are mistaken as foreign by their own immune system. The immune cells surround and attack the base of the follicle, causing it to shrink and become more fragile.
Soon after, it will interrupt its own growth cycle by prematurely pushing developing anagen follicles into the catagen phase before transitioning into the telogen phase (resting).
The underdeveloped hair will characteristically fall out in patches, leaving smooth bald spots.
As long as the hair follicles are still enduring attacks from the immune cells, the bald spots will be left in a dormant state and production of new anagen follicles will slow down drastically.
If the condition is not addressed, it may manifest into alopecia totalis or alopecia universalis, where most or all form of hair growth have halted.
Christiano and her team from Columbia University (the same study aforementioned above) postulated that several immune pathways activate a specific white blood cell called CD8+NKG2D+ T cells.
This T-cell is responsible for the direct attacks on the follicles that lead to the beginning of alopecia areata.
In this extensive study, Christiano and fellow researchers showed that they can prevent these immune pathways from initiating through the use of JAK inhibitors.
In addition, it can reverse the presence of alopecia areata and re-stimulate the follicles back to active anagen phase.
To prepare the subjects, the researchers took CD8+NKG2D+ T cells and recreated the conditions for alopecia areata on the skin of mice subjects.
After a few weeks, the affected skin grafts with spontaneous alopecia areata were transferred onto the backs of healthy mice.
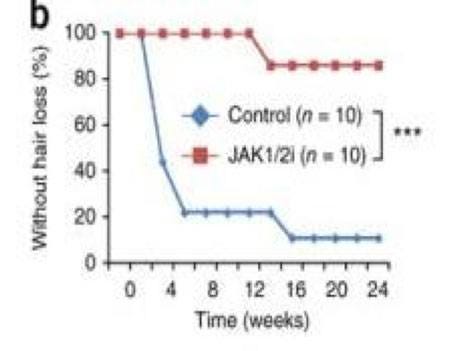
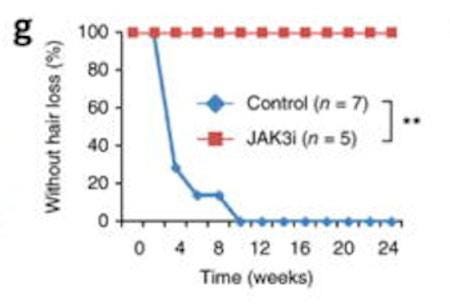
Firstly, to test whether JAK inhibitors would be therapeutically effective in preventing alopecia areata, the researchers administered ruxolitinib and tofacitinib daily on two experimental groups, along with a control group, for 12 weeks.
The results showed that mice on the JAK inhibitor drugs maintained the grafted hair, thus revealing their prevention from the development of alopecia areata and the expansion of CD8+NKG2D+ T cells.
Meanwhile, the control group lost a vast majority of grafted hair after a few months.
Christiano and her team then tested whether JAK inhibitor could reverse subjects that already have an onslaught of the disease.
They took grafted mice that had developed extensive alopecia areata and experimented with daily application of both oral and topical application (on two separate groups) of the drug.
After 12 weeks, while both application methods showed substantial hair growth and reduced the frequency of the CD8+NKG2D+ T cells in treated skin, all of which persisted 2–3 months after treatment stopped, the regrowth for the topical group was stronger and more evident than the oral group.
Researchers were able to observe visible effects as early as 2–4 weeks after the onset of treatment. Within 7 weeks, the mice exhibited full coats of hair and within 12 weeks, complete hair regrowth had emerged following the topical therapy.
In addition, the team noted that untreated areas of the abdomen remained alopecic. They postulate that the topical therapy acted locally and that the observed therapeutic effects were not the result of systemic absorption.
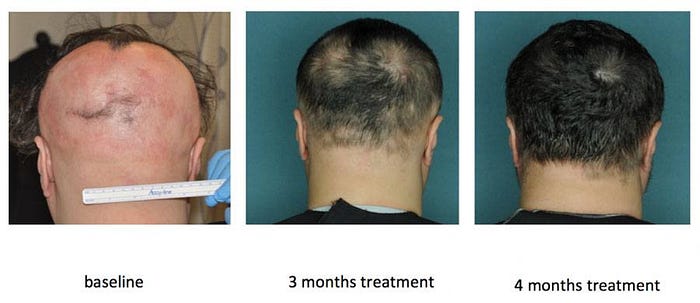
Finally, to test JAK inhibitors success on human subjects, Christiano performed a clinical trial with three patients with moderate-to-severe alopecia areata (defined as more than 30 percent hair loss).
Each patient received 20 mg of oral ruxolitinib taken twice daily for 3–6 months.
As noted above, all three patients achieved near-complete hair regrowth within 5 months of treatment.
In addition, the CD8+NKG2D+ T cells amongst other molecules that were previously harming the follicles showed reduced presence on the scalps.
JAK Inhibitors May Also Work for Other Forms of Hair Loss
In the last study, Christiano and her team were able to demonstrate that hair regrowth was due in part to the reduction of CD8+NKG2D+ T cells infiltration.
However, during the course of the experiment, they were surprised by the unusually robust hair growth in the group that received topical treatment of JAK inhibitor, in comparison to the groups that received oral treatment.
This suggested that there may be other variables at play.
Thus, the researchers conducted a new study that focused on JAK inhibitor and its effect on hair growth cycle. From this, the researchers found several important findings.
1: JAK plays a direct role in influencing the hair follicle’s growth cycle
Mice in late telogen phase (8.5 weeks) were placed into three groups. One group had a control vehicle and ruxolitinib applied separately on divided halves of the back.
Another group was treated with control and tofacitinib, with the same equal division on the back. The animals were only treated for 5 days total before withholding the drug.
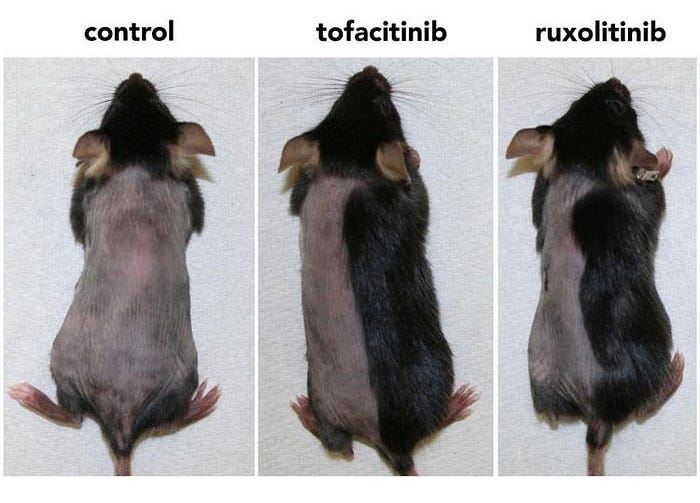
Within only 10 days of starting treatment, approximately 90 percent of the mice treated with ruxolitinib or tofacitinib displayed skin darkening and hair growth, whereas no hair growth was evident in control-treated mice.
Within 3 weeks, the tofacitinib and ruxolitinib-treated skins regrew their entire fur back.
In addition, the researchers treated mice skin in telogen phase with ruxolitinib, tofacitinib, or vehicle control and harvested the skin 5 hours after the first, second, and third treatments.
They found Edu+ cells (important for multiplying hair stem cells) within the drug-treated skin, but not for the control-treated skin.
These findings suggest that JAK normally acts to prevent transition to anagen by encouraging hair follicles to remain in a dormant state.
The suppression of JAK signaling activates a pro-growth/anti-resting signal during telogen, thus allowing for normal hair cycle progression.
2: Hair-inducing effects of JAK inhibition are not dependent on the activity of T-cells/lymphocytes
The hair follicle microenvironment contains a substantial population of resident and migrating T cell, many of which contributes to the maintenance of normal growth cycle.
The researchers took two different types of immunodeficient mice models (lacking specific T-cells and B-cells) and examined whether it made a difference to normal hair growth after treatment with JAK inhibitors.
The results showed that the missing white blood cells did not make a difference to the drug’s response to the follicles, which continued to grow hair robustly.
This suggests that the hair-inducing effects of JAK inhibitors in normal skin are not dependent on the activity of T-cells/lymphocytes. Rather, the vigorous growth of anagen follicles is likely due to an intrinsic property of the hair.
Initially, this may sound conflicting to prior results (remember CD8+NKG2D+ T cells?). But Christiano and her team surmised that when considering hair growth in alopecia areata patients, it is actually a two-step mechanism.
First, the immune attack led by the T cells must be eliminated. Then, the anagen growth must be restimulated.
With this study, they may have proven that JAK inhibitor just has the gift of being able to act on both steps independently.
3: JAK inhibition may help other forms of hair loss
The key to this theory is based on the finding that the elements most directly related to hair growth, such as hair germ, follicular stem cells, and dermal papilla, can be activated directly through the obstruction of JAK.
Many forms of alopecia are characterized by the inability of hair follicles to enter the anagen phase after long dormancy in the telogen phase, such as androgenic alopecia.
By stimulating these key elements, affected hair follicles stuck in telogen phase are given optimal opportunity to enter back into the growth cycle.
However, experts are deeply divided, including Dr. Brett King, and urge many people to remain very skeptical of such bold assertion.
Closing Thoughts
Based on current findings, JAK inhibitor is becoming a serious contender for addressing alopecia areata, and may eventually help other forms of alopecia.
However, interfering with the body’s natural immune system can be dicey business. To no surprise, some serious side effects for oral JAK inhibitor drugs have been reported. Moreover, it is expensive — a 5 mg pill can cost over $67.
While the cream likewise holds a hefty price tag, there is a chance that it may act on the local JAK in the scalp, thus reducing the risk of systemic side effects.
As these are only premature promises, we recommend waiting for additional research on the drug’s safety and efficacy for treating alopecia areata before seriously committing.
Talk to a medical professional before getting started with any hair loss treatment.
